Results of an internet service with home sampling for chlamydia and gonorrhoea infections in Vantaa

Background
In Finland, approximately 13,000 sexually transmitted Chlamydia trachomatis infections are reported annually to the national registry for infectious diseases. The number has not declined despite improved diagnostics and interventions. The threshold for attending a clinic due to a suspicion of chlamydia may be high, especially amongst young individuals. To lower the threshold and thereby enable better control of chlamydia infections we performed a pilot project of an internet service with home-based sampling and central laboratory nucleic acid testing for chlamydia and gonorrhoea. The pilot project was performed in a major city, Vantaa, within the Helsinki capital region by United Medix Laboratories.
Methods
This study was a registry based study concentrating on diagnosis of chlamydia and gonorrhoea infections. The results of the internet service with home sampling were compared with traditional clinic based sampling.
Results
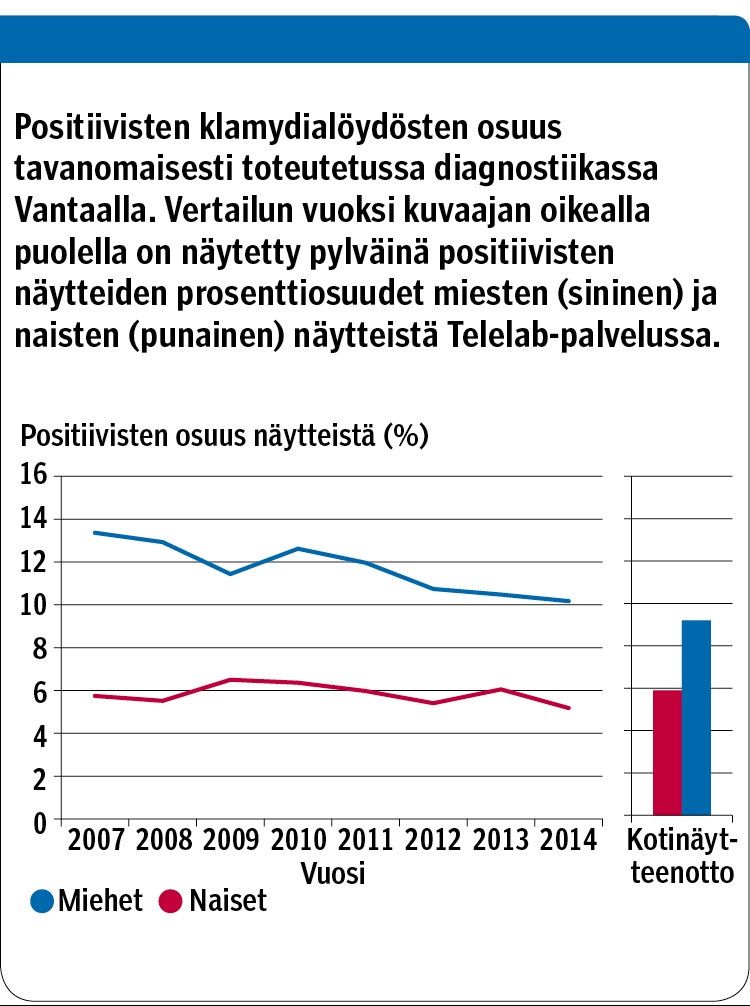
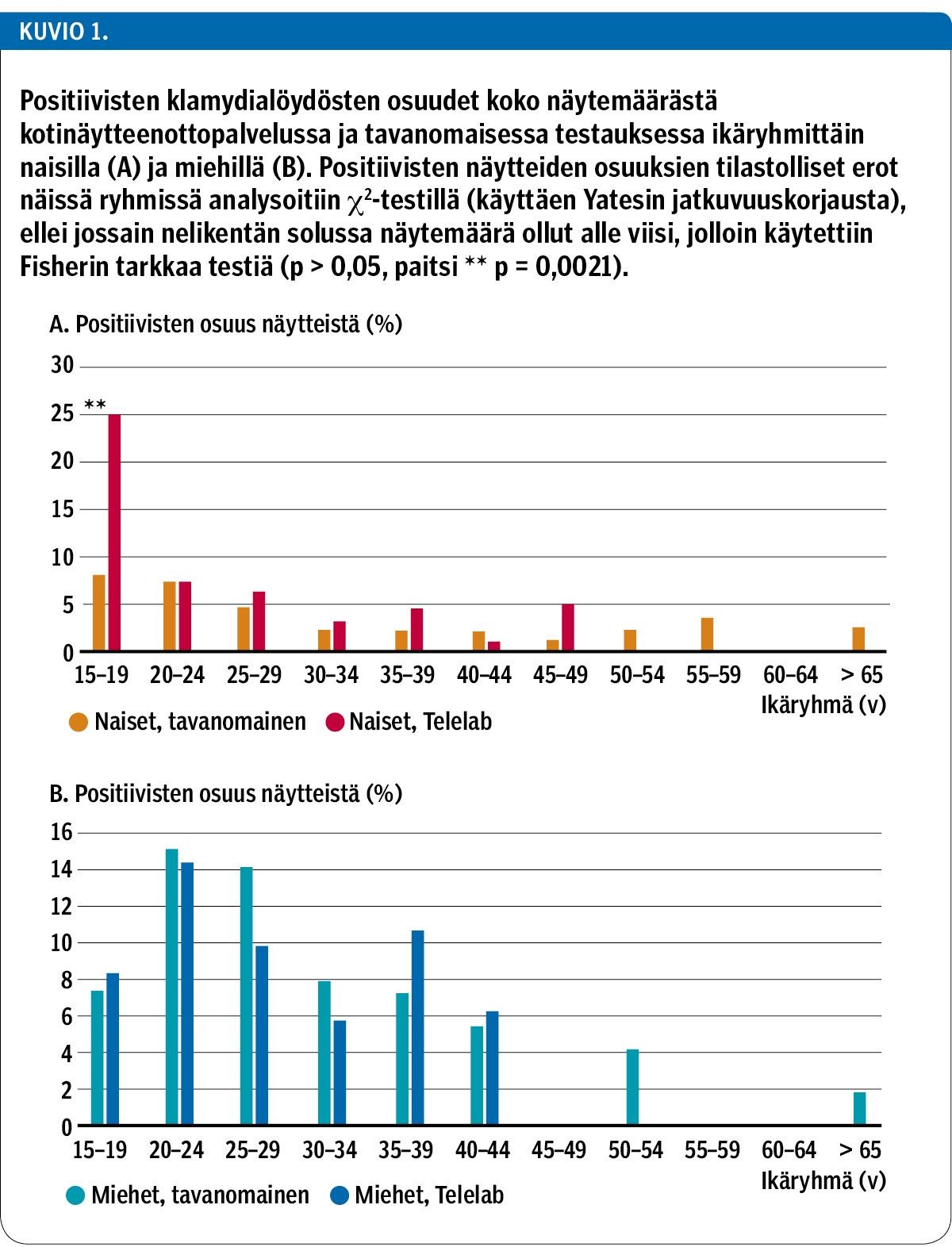
A total of 1550 samples from 1240 patients were received between May 2014 and December 2015. This represents approximately 15 % of all chlamydia/gonorrhoea samples taken during that period in Vantaa. The age profile of the users of the home-based sampling setup was similar to the traditional sampling setup. A total of 5.9 % of samples sent by females and 9.2 % of male samples were positive, corresponding well with the positivity amongst the samples from Vantaa within the past few years. The home-based sampling resulted in higher positivity amongst certain age groups, such as 18–20-year-old females (25 %, n = 44). Gonorrhoea positivity was low (0.06 %). Approximately 17 % of patients repeated sampling after a mean interval of 4–5 months and a significant number of these patients (15–40%) had sent at least one positive sample.
Conclusions
In Finland, an internet service with home-based sampling is also suitable for chlamydia and gonorrhoea diagnosis in a regional setting. The main advantages of home-based sampling are the obviously lower threshold of sampling for certain age groups and the freeing of time of health care personnel from routine sampling to be used for other tasks. On the basis of the results the efficacy of home-based sampling seems to be at least as good as that of traditional sampling while simultaneously providing additional value for certain age groups and anti-chlamydial work.






